I just finished Robert’s latest video and I think a lot of people would benefit if they had a visual aid for the shape of the magnetic field for each type of coil and position.
Not yet, that is immensely complicated to show quantitative magnetic fields in 3-D for all possible configurations, but the rules of thumb are as I have described elsewhere:
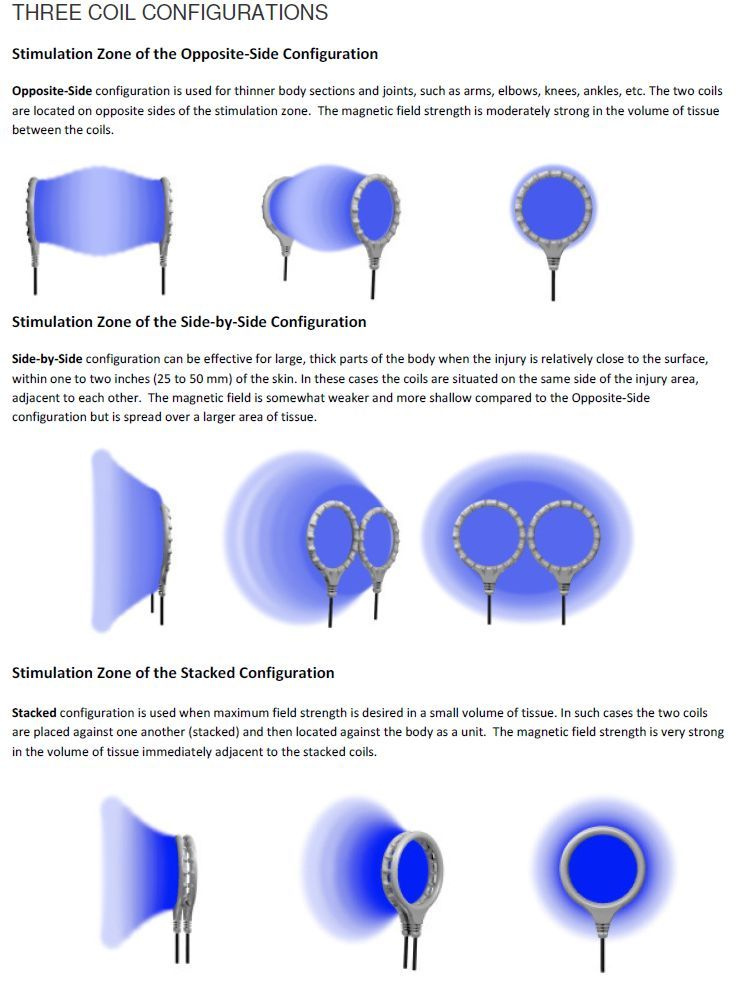
Coils side-by-side, bumps away from the skin:
- resulting field is shaped like a doughnut (torroid) with field lines circulating through the coils, into the skin, through tissues, back out through skin, trough the adjacent coil, out into air, then back into and through the first coil.
Coils stacked, bumpy-sides together:
- Resulting magnetic field is shaped like a mushroom sprouting from each side of the coil stack. Imagine a fountain emerging along the central axis going through the coil stack.
Coils on opposite sides:
- Resulting magnetic field will be (American) football-shaped, with the sharp ends of the football defined by each of the oppositely located coils. The further apart the coils, the wider the football gets, which means less dense magnetic flux lines near the center, which means lower fields.
But, keep in mind, the reason I designed it this way was to make it so that you would not need to spend a lot of time chasing the engineering details of all of this. My strong advice: just try these few different coil configurations for any given injury, then decide for yourself what works best for your individual case. It is not possible to calculate this for any given injury, it is just something you need to determine by experiment because individual tissues and injuries respond differently.
9 Likes
@Bob Great insight! For the opposite coil configuration, what is the maximum effective separation in inches or cm? I’m guessing that beyond 3 inches the magnetic field coupling between the coils is negligible. Do you have any data for the M1 with various intensity settings?
Do you have quantitative data of effective field density wrt M1 intensity settings vs distance for some or all 3 coil configurations? That data would be immensely useful when choosing coil configuration for treating certain injuries and body parts.
As always, thank you for the pioneering work and research you do 
1 Like
That’s the magic question; that’s what I have been working on for 23 years. No one, anywhere, is even close to having numbers pinned down on that.
It definitely looks cool to visualize 3-D magnetic fields, fluid flows, thermal gradients, distortions of space and time, all that stuff. But doing so in the case of PEMF can be very misleading. Basically, it presents the wrong stuff and because makes it look like hard science, it leads to the marketing fraud problem that we currently have.
The best anyone, anywhere, can possibly do at this point is collect as many clinical/anecdotal observations as possible, then put together a list of “what seems to work” versus “what does not work”, basically a list of rules of thumb.
So, I will begin with the rules of thumb:
Everyone responds as an individual (biological sensitivity to electromagnetism), so there is no one number for anything that defines “enough to work” versus “not enough” versus “too much”.
Field density is the wrong number to quantify. If all you need is high magnetic field density, then you just need to buy a strong magnet for about $1. Of course, we know these do not work. You need a magnetic pulse waveform of the correct shape, duration, and amplitude. This makes the calculations many billions of times more complex (watch for a paper to be published on this in the next few days, I will try to post it here)
So, before we slip back down the rabbit hole of too-complex-math-biology-and-physics, we need to pull back and say the best answer possible at this time is to follow the basic rules of thumb that I have posted many times:
1st: you need to try a few variations, and observe carefully, to see what works for you. I have already done my best to have enough power and flexibility to make it effective for almost everyone. It usually only takes a few days to do some self-experiment to find what works best for you as an individual.
It usually takes three or four tries to get coil placement right for you.
Try stacked, versus side-by-side, versus opposite side coils. Depth of field penetration is less important than magnetic field line direction (orientation), because it is well established in the scientific literature that the biological response depends upon direction of ion flow, which depends on the E-field gradient vector, which is calculated by vector calculus based on the first time derivative of the B-field vector. That’s about as simple as you can make it. Just measuring the magnetic field density by itself does not even start to tell you the right answer.
Summary: magnetic field direction is at least as important as magnetic flux density, but both are far less important that the rate of change of the magnetic field as calculated in three-dimensional space.
Then there is the fact that inductive coupling with ionic species/fluids in the tissues actually changes the nature of the magnetic field because inductive coupling results in energy transfer to the tissues (this is what causes the biological effects), which means the shape of the waveform will begin to become distorted…
CAUTION, another rabbit hole dead ahead.
After decades of working on this, I think the most practical answer is:
Coils: try stacked, side-by-side, then opposite side coils, in that order, directly over where it hurts.
Move the coils around a bit to reorient the magnetic field to find what works best for you and your injury.
Pay attention to how you respond; take notes.
Start with standard settings (Omni-8)
Start with medium intensity (about 9)
If after this you feel that you really need deeper field penetration (that is rarely the case), then you can try:
-coils on opposite sides with different orientations around the point of interest
-our deep field coil assemblies using a C5
-Stack and tape individual coils and use them on opposite sides
Too much intensity generally is less effective for most people; dial it down a bit and observe changes.
If you do these things (above), you will find a configuration that works well for you almost all of the time, usually in just a few days.
If you try to calculate your way to an answer, you will spend decades (as I have) and millions of dollars (as I have) and you might arrive at the same answer.
Happily for everyone , I have already spent the time and the money, and the answer is:
See the rules of thumb above.
9 Likes
Thank you for the detailed semi-technical (limited rabbit holes  ) answer. As usual it makes sense Evidently it falls a bit short of the numeric answer I was dreaming of
) answer. As usual it makes sense Evidently it falls a bit short of the numeric answer I was dreaming of 
My seeking a practical numeric answer was due to the fact that I have been treating a femoral neck fracture (if you recall from a previous post). When treating this type of injury as you know, pain is not the indicator being sought, but rather, bone healing shown on X-rays. Due to the typical 3 month period between imaging, the price of not getting an effective or the “optimal” coil placement, arrangement and intensity can be the difference between 2-3x accelerated healing to 0 
In my use of PEMF for my injury, I hit it from every angle I could think of, with 90% stacked coils configuration as I assumed (perhaps incorrectly) that higher intensity would be required to reach the entire broken bone area. I didn’t use much of the opposite sides coil configuration (perhaps in error once again) due to the 6-7" span from front to back of hip (ya, I’m a pretty skinny guy). I hit it from the top, bottom, side and outer side angles. I also varied treatment time every few weeks as I’m sure that is another significant variable on effectiveness.
The outcome thus far has been comparable to a 1x healing time from a clinical empirical data point of view. My 13 week X-ray still showed incomplete bone healing. My next data point will be in mid-May.
I do nonetheless accept and understand that there are many many variable at play here as I name a few: my current rate of healing at the youthful age of 49, amount of movement, exercises and weight bearing during healing at various stages just to name a few, on top of the ones you mention on the PEMF side. Given all of these, possibly I healed very fast compared to not having used PEMF at all. But, I have no data to confirm nor disprove this statement.
So, we continue to gather data and share experiences and outcomes in the search of optimal (or at least incremental) benefit.
P.S. I’m collecting data and imaging to update my injury post to share further on my experience.
1 Like
OK, so the challenge here is that you do not have an easy metric (such as pain relief) to base your feedback decisions on. And as I was saying, there is unfortunately no way to calculate a solution, such as: “A-B-C will work, but X-Y-Z will not”.
A femoral neck fracture is another challenge: that is about as deep as you can get unfortunately.
So the next best thing we can do for you is to try to use our best judgement, and I can definitely help with that. The advantage we have is that you do not need a generic answer such as “this and that will be effective at such-and-such a depth”. While it would be convenient, I agree with you, it is not very realistic unfortunately. In your case we can think about a specific injury at a specific anatomic location, given the specific geometry of your individual body size.
This is where specific, individual conditions really drive the decisions. For example, since you have a 6" to 7" span from front-to-back of your hip, then that changes my calculations quite a lot. That effectively simplifies the depth-of-penetration problem. Depth is definitely not the issue here.
Also, keep in mind that you do not need to completely cover a tissue with a magnetic field to be effective; just treating adjacent tissues clearly has very positive spill-over effects.
Also, you are doing a lot of different things (using different angles for coil placement), which is generally an excellent strategy.
Also, let’s consider what we think we know about your specific situation. If you are healing well at all, all things considered (age, injury type and severity, etc.) then I would say you are fortunate. Based on a lot of observations and clinical feedback, I would definitely think that you are benefiting from using PEMF. As you point out, it is impossible to say for sure with data, but it is reasonable to conclude that you have probably benefited.
My current thinking is that the primary considerations in your case are (in rank order starting with the most important):
1–direction of the magnetic field lines of the pulses. For bone fractures in particular, this is critical, because bone healing rate depends very much on the direction of the electrical current flow with respect to the long axis of the bone. This has been published since about the 1960’s. The electric current flow direction depends on the magnetic field line direction, which depends on the orientation of the coils.
In your case, I am thinking that to get the right magnetic flux vector (specifically the direction along the bone) you want to try coils on opposite sides, or maybe stacked (less likely), but probably not side-by-side.
2–I would keep the intensity to about 11 - 12, not really maximum.
3–I would use a pulse pattern that includes both fast and slow pulse rates, such as the Omni-8 or A9. I would change the pattern every few days, maybe to alpha-wave, for example.
4–You might also try changing the opposite-side coil placement, from front-back to inside-outside (medial-lateral) if you can position the femoral head break approximately between the coils.
Another trick, that I think you are already doing, is to change things up from time to time. You might even try changing things up at different times of day, every day. The theory is that incorrectly placed ICES-PEMF coils have less benefit, but not negative benefit. Thus, by varying the coil placement, you will occasionally get things optimally placed and will benefit from that, whereas sub-optimal placement will only be sub-optimal, not damaging.
And since PEMF has persistent beneficial effects, if you have the coils placed correctly at least some of the time, then you get about the same benefit as having them placed correctly most of the time.
This is the same logic I go through for myself with serious injuries, or when I am helping a clinician develop a strategy for helping someone else with a serious injury that has not responded to other approaches. If you think along these lines, I would say that your chances for good benefit from ICES-PEMF are very high.
6 Likes
A side note on coil placement. I have a wrap with stacked coils taped to it. I’ve used this many times and noticed that the batteries consistently last quite bit longer than usual. There seems to be some kind of coupling effect that results in less drain on the battery. I have no idea what this might signify, if anything.
3 Likes
It may be that holding the cables more stably in place reduces any effect of a minor transient short circuit. As I am testing different coil designs, and as they wear out, I see the same effect: taped up or otherwise held firmly means longer battery life.
5 Likes
@patient9, not sure why I missed these pictures before, but, under the replacement coil product page the following illustrations are available and should be exactly what you were looking for
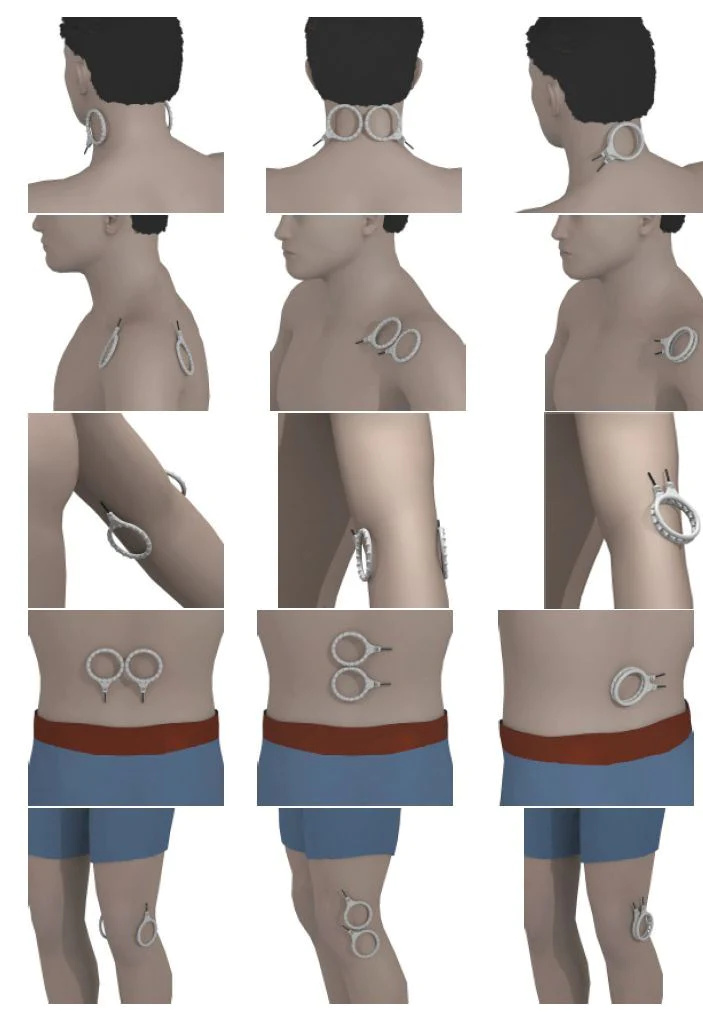
2 Likes